I discuss issues pertaining to the practice of neuropathology -- including nervous system tumors, neuroanatomy, neurodegenerative disease, muscle and nerve disorders, ophthalmologic pathology, neuro trivia, neuropathology gossip, job listings and anything else that might be of interest to a blue-collar neuropathologist.
Jeremy Deisch, M.D., a neuropathology fellow at the UT Southwestern Medical Center in Dallas, recently emailed to inform me that he has begun a pathology blog which focuses on neuropathology and forensic pathology. So far, Pathwonk has gotten off to a great start! Dr. Deisch's most recent post features Loma Linda University's Neuropathology Museum. Cyril Brian Courville, M.D, a neurologist, neurosurgeon, and neuropathologist, who was the chairman of the Loma Linda University Department of Nervous Diseases, as it was known at the time. Regarding his blog, Dr. Deisch writes: "My intent is to share interesting cases which come through our department, most likely on a weekly basis. I also aggregated some links to websites and files that I found useful as both a pathology trainee and as a NP fellow. Right now, my focus is on NP. I'll be doing a forensic fellowship next year, so I'll probably put some non-NP autopsy cases in as well." Best of luck, Dr. Deisch, and welcome to the blogosphere!
The next in our Best of the Month Series is from July 2, 2010:
Recent neuropathological autopsy findings of a 26-year-old NFL player lend further credence to the idea that perhaps our high school children should not be playing football. Former Cincinnati Bengals player Chris Henry, who died after falling from a moving pick-up truck during a fight with his fiancee, was found to have histomorphologic evidence of chronic traumatic encephalopathy (CTE). See the tau-immunohistochemistry photomicrograph from Henry's brain above. The findings consist of neurofibrillary tangles similar to those seen in Alzheimer disease. This CNN.com article raises the question in my mind of whether school districts should offer genetic testing to potential players, as one's apolipoprotein E genetic status seems to indicate the likelihood that one might be more susceptible to the development of CTE. In any case, I intend to forbid my own son from playing football and from boxing. Any other sport is fair game. But I will not allow him to a participate in a sport where head injury is intrinsic not only to playing the game, but even participating in practices. This is not to say that I'm some kind of a pansy who is averse to any risk. I will allow my child to play any other sport, as head injury in other sports occur merely as accidents. But football and boxing will remain off-limits in my home.
As I mentioned before on this blog, I am indebted to Sherry Miller, wife of neuropathologist Doug Miller, MD, PhD, for keeping me updated on neuropathology job openings. As a result, Neuropathology Blog has the most up-to-date and comprehensive listing of neuropathology job openings on the web. And there are a lot of jobs available! Sherry recently wrote me the following email regarding the current status of the neuropathology job market: "What do you think is going on? A shortage? People leaving and moving around? Adding staff? (I don't think this is likely as most places are cutting staff.) There are 28 jobs posted on the blog...now even if 6 are out of date because people haven't responded to the emails, that still leaves an incredible number of vacancies..... Maybe that would be a GOOD blog post? Ask what others think is going on?" I agree, Sherry. That WOULD be a good blog post. The floor is now open for comment......
Today's guest post is from Dr. Zahid Kaleem, hematopathologist at Missouri Baptist Medical Center.In collaboration with other pathologists, Dr. Kaleem has created a website called Pathpedia.com, which will enhance exchange of ideas and interesting cases among neuropathologists as well as those who deal with the "lower organs". It's exciting to see yet another colleague joining the ranks of pathologist social networkers. Here's Dr. Kaleem's post:
Pathpedia.com is a comprehensive web-based resource on human anatomical, clinical, and experimental pathology. The site serves a target audience including pathologists, pathologists-in-training, laboratory professionals, clinicians, medical scientists, and medical students. For neuropathologists, the sites offers listing of annual meetings and educational courses from around the world, postings of unusual pathology cases, a browsable table of content of various neuropathology/neurology journals, the ability to create your own WikiBook, and the opportunity to post jobs and resumes. Soon to be released is a listing of CME / SAM, both paid and free, in all specialties including neuropathology.
Thanks to Dr. Peter Cummings forwarded my this article from the New York Times about a a new book of images of the brain using the latest in computerized imaging techniques. I was struck by one image in particular:
The above image shows the basic organization of the human visual cortex. The New York Times article states: "Data from a functional M.R.I., obtained in a live human subject, illustrate the basic organization of our primary visual cortex, in which neighboring points in a visual scene are mapped to neighboring points on the brain. Visual stimuli far from the center of the gaze are processed in the areas colored dark blue, while visual stimuli in the center of the gaze are processed in the areas colored purple."
Credit: Jack Gallant
Data from a functional M.R.I., obtained in a live human subject, illustrate the basic organization of our primary visual cortex, in which neighboring points in a visual scene are mapped to neighboring points on the brain. Visual stimuli far from the center of the gaze are processed in the areas colored dark blue, while visual stimuli in the center of the gaze are processed in the areas colored purple.
Another excellent neuropathology job is available in the San Francisco Bay Area with Dr. Hannes Vogel. (Dr. Vogel is pictured with a ribbon just after finishing the Western States 100 Mile Endurance Run with a time of exactly 23 hours, 49 minutes, and 55 seconds along with "Team Vogel", including Vogel's wife of one week, Monique, immediately to his right. Most readers will recognize Dr. Greg Fuller of MD Anderson Cancer Center at the far right, who came to the event all the way from Houston). Stanford is seeking a neuropathologist with interest in neurodegenerative disorders. Here are the details:
The Department of Pathology at Stanford University School of Medicine seeks an academic Neuropathologist with a research interest and a record of accomplishment in the area of neurodegenerative disorders for appointment at the rank of Assistant, Associate, or Professor in the Medical Center Line or University Tenure Line. Faculty rank, and whether the appointment is made in the Medical Center Line or University Tenure Line, will be determined by the qualifications, experience, and interests of the successful candidate.
Neuropathology handles each year approximately 800 neurosurgical specimens from Stanford University Medical Center (SUMC), and an additional 600 consultation specimens from outside of SUMC, including over 300 muscle biopsies from SUMC and non-SUMC patients; the service also is responsible for approximately 250 brain examinations annually. Duties will include sign-out responsibilities in surgical and autopsy neuropathology, including frozen section analysis, but the amount of time spent on clinical responsibilities will be greater if the individual is appointed in the Medical Center Line than for one appointed into the University Tenure Line. It is expected that the successful candidate will serve as the participating neuropathologist on program and core grants in the area of neurodegenerative disorders. If the successful candidate is in the Medical Center Line, she or he also will contribute to the expansion of our diagnostic services in neuropathology to those outside of SUMC, through our consult service. Candidates must hold an M.D. or an M.D., Ph.D. and board certification in anatomic pathology and neuropathology, and are required to hold or to be eligible for a current license to practice medicine in the State of California.
The successful candidate will be expected to lead and/or contribute to clinical, translational and/or basic research projects and to participate in training clinical residents and fellows. Departmental support is available for suitable research projects by Medical Center Line faculty, whereas University Tenure Line faculty are expected to derive a substantial portion of their salary and research support from extramural sources. Applicants should submit curriculum vitae, as well as a brief description of research accomplishments and plans for future research. These, with the names of three references, should be sent to:
Stephen J. Galli, M.D.
Professor and Chair
c/o Ms. Cynthia L. Llanes
Department of Pathology
Stanford University School of Medicine
Stanford, CA 94305
E-mail: cllanes@stanford.edu
Since his recent move to the University of California San Francisco, Dr. Arie Perry (pictured) is already looking to expand the neuropathology division. See below for a great opportunity for the right neuropathologist!
SAN FRANCISCO, CALIFORNIA (USA). The Department of Pathology and the Institute for Neurodegenerative Diseases (IND) at the University of California San Francisco is seeking an outstanding candidate for a full-time faculty member with research, clinical service and teaching responsibilities at the Assistant, Associate or Full Professor level.
The successful candidate will direct his/her own basic or translational research program and will become an integral member of the large multidisciplinary team at UCSF involved in both clinical and collaborative research activities related to neurodegenerative disorders. Additional resources are also available in the Memory and Aging Center at UCSF, the Gladstone Institute of Neurological Disease, the Program in Biological Sciences (PIBS) Neuroscience Graduate Program and the Biomedical Science (BMS) Graduate Program. The candidate will be actively involved in teaching fellows, residents and medical/graduate students and must be willing to participate in departmental and interdepartmental conferences. Candidates must have an MD, valid California medical license and be Board Certified (or board eligible at appointment time) in Anatomic Pathology and Neuropathology. Special consideration will be given to candidates with research interests related to Alzheimer disease, Parkinson disease, frontotemporal lobar degeneration or other currently recognized tauopathies, including chronic traumatic encephalopathies. Salary and appointment rank will be commensurate with the applicant's experience and training.
UCSF seeks candidates whose experience, teaching, research or community service has prepared them to contribute to our commitment to diversity and excellence. UCSF is an affirmative action/equal opportunity employer. The University undertakes affirmative action to assure equal employment opportunity for underutilized minorities and women, for persons with disabilities and for covered veterans.
Applicants should submit a curriculum vitae, and three letters of recommendation within one month of the appearance of this announcement to:
Arie Perry, MD
Professor of Pathology and Neurological Surgery
Re: Search #M-3372
C/O Shirley McFaden, Personnel Manager
University of California San Francisco
185 Berry Street, Suite 100, Box 0506
San Francisco, CA 94143-0506
Email: Shirley.McFaden@ucsf.edu
The next in our Best of the Month series is from June 29, 2010:
The Diagnostic Slide Session at the recent American Association of Neuropathologists annual meeting in Philadelphia featured a fascinating case by Dr. Sandra Camelo-Piragua, Ronald A. Goerss, and David N. Louis of Massachusetts General Hospital. The case was that of a 38-year-old AIDS patient who had been only intermittently compliant with his HAART therapy. He presented to the hospital with seizures in 2009 after a year of fluctuating neurological symptoms. Imaging studies showed the following white matter changes:
Biopsy showed a marked lymphocytic infiltrate, which included diffuse, perivascular, and follicular arrangements:
Macrophages were also present:
The following stains for organisms were all NEGATIVE: AFB, GMS, HSV1, HSV2, CMV, HHV8, and toxoplasma. An H&E/LFB stain demonstrated that this was a leukoencephalopathic process:
Immunohistochemistry of one of the lymphoid follicles indicated that the lymphoid infiltrate was a reactive, rather a neoplastic process:
Polyoma virus immunohistochemistry for the SV40 (a surrogate marker for JC virus due to cross-reactivity) was found to be positive:
So, the final diagnosis rendered was Progressive Multifocal Leukoencephalopathy (PML) with concomitant Immune Reconstitution Inflammatory Syndrome (IRIS). IRIS is an inflammatory response in HIV-infected individuals upon initiation of HAART therapy. The immune response can be so robust as to cause morbidity, particularly with the brain is involved. Thanks to Dr. Camelo-Piragua for providing the images associated with this interesting case, and I wish her the best of luck in her upcoming move to Ann Arbor where she will take a position on the faculty at the University of Michigan!
I featured Dr. Sandra Camelo-Piragua this past June because of the interesting case she presented at the AANP diagnostic slide session. Dr. Camelo-Piragua has emerged from her neuropathology fellowship at Mass General and is a newly minted staff pathologist at the University of Michigan! Congratulations, Sandra! With her permission, I am reproducing an email I recently received from her. If you can help her in her quest, please write back to her directly or post a comment. Thanks!
Dear Friends and Colleagues:
I am interested in buying a couple of muscle and nerve pathology books that are currently out of print in their editorial houses:
Pathology of Skeletal Muscle by Stirling Carpenter and George Karpati Oxford University Press, USA; 2 edition (January 15, 2001)
ISBN-10: 0195063643
ISBN-13: 978-0195063646
Atlas of Peripheral Nerve Pathology by R.H. M. King A Hodder Arnold Publication; 1st edition (July 15, 1999)
ISBN-10: 0340586664
ISBN-13: 978-0340586662
Please let me know if anybody is interested in selling a second hand copy that you are not currently using or if anybody knows where I can purchase them directly.
The next in our Best of the Month series is from May 13, 2010. Free samples of IDH1 may or may not still be available, but you can check with the company:
Dianova, the German company that makes anti-human IDH1 antibody for use in immunohistochemical staining of gliomas versus gliosis, is providing free samples of its product. Just go to the site, click on "free sample", and make a request via email. This marker may well be a tremendous advancement in distinguishing reactive astrocytosis from diffuse astrocytoma, so I would encourage you to get your free sample! Thanks to Drs. Craig Horbinski and Ty Abel for assisting me in discovering this opportunity.
USA Today ran a story today about a simple blood test that the US Army has developed which may objectively test for the presence of concussion. The Army collaborated with Banyan Biomarkers, a Florida-based company, to develop the test. In checking Banyan's website, it looks as though the test consists of a panel of immunoassays which include SBDP145, SBDP120, UCH-L1, MAP-2, GFAP. If this test turns out to be as good as the Army is implying, the implications for those on the battlefield (and on the football playing field, I might add) are enormous. If it pans out, I would agree with Gen. Peter Chiarelli, the Army vice chief of staff, who is quoted in the article as saying: "This is huge."
This is a guest post by Amanda who writes on behalf of the San Diego Gamma Knife Center, a shared resource for the San Diego neurosurgical and radiation oncology community.
Gamma Knife surgery has become one of the most popular and extensively tested types of what is known as “stereotactic radiosurgery”, or SRS. SRS (as depicted in the accompanying illustration) is a non-invasive medical procedure that uses highly focused radiation beams as a treatment for brain tumors and other kinds of intracranial maladies. Gamma Knife surgery has been used for treating trigeminal neuralgia, and the treatment of both benign and malignant brain tumors. But the Gamma Knife is not the only SRS system available. In recent years, the popularity and acceptance of radiosurgery procedures has led to the development of newer SRS systems. The most well known among these newer systems is the Cyber Knife. Both the Gamma Knife and the Cyber Knife can be highly effective in treating many of the same maladies, but they operate on patients in fundamentally different ways. Here is a brief comparison of the two SRS systems.
How They Work
During Gamma Knife surgery, patients undergo a CT scan and sometimes also an MRI scan prior to the actual procedure. These scans are used by a team of specialists to plan out the radiosurgery in minute detail. Once the planning is finished, the patient is brought over to the Gamma Knife table and his/her head is fixed onto a rigid head frame that automatically positions the target area of the brain in the spot where the radiation beams will intersect. The Gamma Knife system then delivers approximately 201 highly focused cobalt-60 source radiation beams into a single target area of the brain. The beams are delivered all at once, multiple times and in short bursts. The procedure can last as little as 30 minutes and usually a single session is all that’s needed to complete the treatment.
Unlike the Gamma Knife system, which is designed exclusively for use in non-invasive brain surgery, the Cyber Knife system is designed to conduct SRS on lesions anywhere in the body, including organs that move with the patient’s respiration. It can do so because, unlike the Gamma Knife, it does not deliver the radiation beams to the target area simultaneously. Rather, it uses a single, high-energy photon beam that’s attached to a robot arm. The arm moves to different positions during the surgery, aiming at the target area from different angles. A head frame is not necessary either. Instead, patients are secured to the treatment table with a plastic mask that helps the Cyber Knife update the position of the skull in real time, allowing the robot arm to compensate for patient movement. More than one treatment session is sometimes required.
Accuracy and Efficiency
Both systems can be highly effective in the treatment of brain tumors and other intracranial maladies, but the Gamma Knife has a slight advantage when it comes to accuracy (0.5mm or less, as compared with the Cyber Knife, which can have an accuracy of almost 1mm). Also, the smaller size of Gamma Knife collimators makes it less likely that healthy brain tissue surrounding the target area will be damaged during surgery. The advantage of the Cyber Knife, however, is that its guided robot arm allows it greater versatility to treat other areas of the body and certain regions of the brain that are more difficult to treat using the head-frame method of the Gamma Knife.
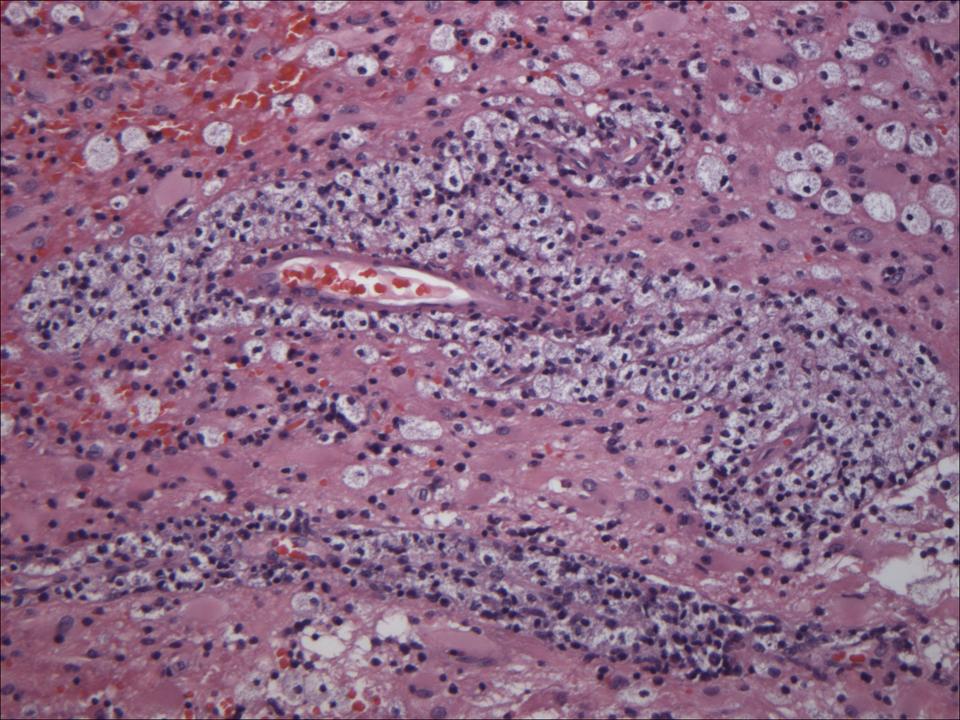
... or does everyone see extramedullary hematopoesis in the majority of their chronic subdural hematoma specimens? Here's yet another example that landed on my desk today:
The next in our Best of the Month series is from April 28, 2010:
You may be surprised to learn that the infamous Walter J. Freeman,
MD (1895-1972), America's most prolific frontal lobotomist, was once president of the American Association of Neuropathologists. The AANP website lists Dr. Freeman (pictured) as having been president of the organization in 1946.
If you want to learn more about Dr. Freeman, get hold of a PBS documentary called The Lobotomist, which explores the background of the procedure popularization during the 1940’s through the ‘60’s. The neurologist Walter J. Freeman of Washington, DC was primarily responsible for the widespread performance of this surgery in the United States by developing the 10-minute, outpatient “ice pick lobotomy”. An ice pick-like instrument was inserted beneath the eyelid and over the eyeball of a patient who was rendered temporarily unconscious by electroshock. (The photo below from 1960 depicts the procedure performed on 12-year-old Howard Dully whose stepmother complained of the child's chronic misbehavior). When the instrument hit the thin orbital plate of the frontal bone, a few taps with a mallet would allow entrance into the intracranial cavity. The ice pick was then advanced upward, after which it was swept back and forth like a windshield wiper blade. The instrument was then extracted and the procedure was repeated on the opposite side. Approximately 30,000 of these procedures were performed before the medical establishment decided that it was ill-advised.
These procedures were designed to sever the connections of the brain with the prefrontal cortex. The goal was to leave patients with a degree of abulia, but with no focal deficits.
The next in our Best of the Month series is from March 11, 2010:
I was recently sent a specimen from the cerebellum of a 27-year-old female patient who, during a routine funduscopic exam at her optometrist, was found to have papilledema and retinal hemorrhages. She was completely asymptomatic -- which of course suggests that we are dealing with a slowly progressive process. A head MRI was obtained:
An image-guided craniotomy ensued, yielding a cerebellar specimen. Photomicrographs of that specimen, at progressively higher magnification, follow:
The top picture exhibits normal cerebellar cytoarchitecture on the right giving way, on the left, to an internal granule cell layer that has transformed into larger gangliocytic neurons. The bottom picture demonstrates the cytologic appearance of these transformed ganglion cells.
This is an example of dysplastic cerebellar gangliocytoma, otherwise known as Lhermitte-Duclos disease (LDD). Dr. Peter Burger and colleagues, in their Surgical Pathology of the Nervous System and Its Coverings (4th edition, page 274), make this comment about LDD: "In the parlance of bird-watching, an endeavor with many similarities to surgical pathology, Lhermitte-Duclos disease is an entity not likely to be found on the 'life-list' of most pathologists." Well, this rara avis is now on my life-list!
When I came upon this tumor, I immediately thought of Dr. Ty Abel(pictured to the left), neuropathologist at Vanderbilt, who in 2005 authored an immunohistochemical study of 31 cases of Lhermitte Duclos disease. I emailed him this question: "What is the current thinking on LDD? Is it a hamartoma or a neoplasm or something in between?"
Ty's response: "Something in between may be the best answer. We suggested in our paper that it was a 'hypertrophic phenomenon superimposed upon a developmental malformation'. Our observations, as well as those in Suzie Baker's mouse model of this, suggest that aberrant signaling in the pathway disrupts granule cell migration as well as leading to their hypertrophy. Histologically, there is little proliferation, so the increase in tumor size over time may be due to cellular hypertrophy or to the abnormal myelinization of the molecular layer or both.Still, they do grow and sometimes come back after resection, making them tumor-like. Does your patient have evidence of Cowden's?"
No, my patient does not have other clinical evidence of Cowden syndrome. But Ty put me in touch with a leading authority on Cowden syndrome at the Cleveland Clinic, Dr. Charis Eng(pictured to the right) who emailed me this comment: "What we found in our initial series is that adult-onset LDD is almost always associated with germline PTEN mutations, i.e., has Cowden syndrome."
Whether or not this patient gets germline PTEN testing, she should be closely surveilled for breast, thyroid, and endometrial cancer, as there is a high incidence of these tumors in patients with Cowden syndrome.
And now a recut slide of this rare bird gets filed away in my teaching set, only to be let out of its cage again by the eager inquiry of a resident.
The Huffington Post reports today on the suicide of a University of Pennsylvania football player. Neuropathologists at Boston University performed a brain autopsy which showed chronic traumatic encephalopathy (CTE). The New York Times also reported on this case. The young football player's mother wanted to make the results public, saying "there's nothing trivial about this whatsoever. Anyone who thinks that this can be swept under the carpet is in for a big shock. It's a big implication here." The implication being, of course, that CTE contributed to the young man's depression which, in turn, led to his suicide. "How can you blame football for the kid's suicide?", one might ask. I don't think anyone is making that kind of simplistic connection. There is evidence that the young man had brain damage, and one might infer that it came from playing football. Perhaps brain trauma in an individual who is genetically predisposed to CTE may be a contributing factor leading to suicide. That speculation alone ought to be enough to make parents think twice before enrolling their kid in a football program.
The University of Maryland School of Medicine, Department of Pathology invites applications for a Neuropathologist at the academic rank of Assistant Professor. Academic appointment and salary will be commensurate with experience and qualifications. Applicants must be board certified (or board eligible) in Anatomic Pathology and Neuropathology.
Clinical responsibilities in Neuropathology (shared with others) include intraoperative neurosurgical consultation and permanent section interpretation, muscle and nerve biopsy interpretation, autopsy brain examination and neuropathology consultation from a number of hospitals. Additional responsibilities may include the diagnosis of general surgical pathology specimens and participation in the autopsy rotation and outreach pathology activities.
The applicant will have demonstrated an academic active interest in basic or translational research, with a strong record of publication and an interest in teaching. Additional responsibilities include teaching of medical students, residents, fellows, graduate students and students in our Pathologists’ Assistants Program.
The University of Maryland School of Medicine is the fifth oldest and first public medical school in the nation and is the founding school of the University of Maryland. The School of Medicine ranks in the top tier of medical schools nationally and has approximately $425 million in research grant awards and contracts.
Applicants should forward their curriculum vitae, a brief statement of their scholarly and research interests and the names of three references to:
Sanford A. Stass, MD
Professor and Chair
Department of Pathology
University of Maryland School of Medicine
c/o Pati Butler (pabutler@som.umaryland.edu)
10 South Pine Street, MSTF, Room 7-00
Baltimore, Maryland 21201
This guest posts was authored by Dr. John E. Donahue, neuropathologist at Brown University School of Medicine. Dr. Donahue (pictured) is responding to a question raised by a neurology resident who considering doing a neuropathology fellowship. I would argue that, despite the potential professional hurdles such cross-training might present to the trainee, neurologists who practice neuropathology bring a fresh insight which dynamizes the subspecialty. Here are Dr. Donahue's thoughts :
I am a neurology-trained neuropathologist. Many years ago, that was the norm; almost all neuropathology was done by neurologists. They saw patients, cut brains, looked at slides, and taught. Mass. General Hospital had neurology, neuropathology, and psychiatry as a single department until the late 1950's.
Nowadays, the neurologist-neuropathologist is going the way of the dinosaur, and I may be one of the last of my kind. Neuropathology has been taken over by pathology in most places, and almost all neuropathologists are now pathology-trained. For those that are still in medical school and contemplating neuropathology, as much as it breaks my heart to say this, I'd strongly consider going the pathology route from a pragmatic perspective. In the 21st century, it's much easier to find a job this way. For those that are already in a neurology residency and have their heart set on neuropathology, there are four distinct job possibilities that come to mind. A certain amount of teaching, either to medical students, residents, fellows, or all of the above, is a requirement for most jobs in all of these categories.
1) Neuropathology (NP) only. This is what I thought I was signing up for when I signed up for NP because the neuropathologist where I did my neurology residency did NP only. However, come to find out, these jobs are extremely rare. It would require being in an academic setting with a big enough neurosurgical volume to justify the expense of an NP-only person. This is not a realistic possibility for most jobs.
2) NP/neurology. Very few places have neurology and NP in the same department. The New Jersey Neuroscience Institute in Edison, NJ comes to mind as one. However, in the vast majority of institutions, NP is under the domain of pathology. Thus, in order to pull off the NP/neurology combo, a lot of administrative creativity and flexibility are required. You'd have to be paid by two departments and be beholden to two chairs. Like NP only, this is not a realistic possibility for most jobs.
3) NP with anatomic pathology (AP). In order to be board-certified in NP via the neurology route, in addition to the two-year NP fellowship, you have to do a minimum of one year of an AP residency. If you do a second year, that would make you board-eligible in AP as well. This would significantly increase your marketability and the number of pathology employers that would potentially be interested in hiring you. In the 21st century, if you have your heart set on NP and don't mind examining "lower-organ" pathology, this would be my recommended route to the best job security. Keep in mind that if you go this route, you're looking at EIGHT years of residency and fellowship after medical school graduation (one year internal medicine, three years neurology, two years NP, two years AP). Can you tolerate being a trainee for that long?
4) NP-research. If you have your heart set on neuropathology, hate "lower-organ" pathology, and/or don't want to spend eight years as a clinical trainee, then you most likely will have to go this route. The only way for neuropathologists to generate substantial amounts of revenue without having to do AP is to bring in research grant money, either from NIH, private foundations, industry, or any or all of the above. So you'd best attach yourself to a mentor during your residency and learn how to do basic neuroscience research, generate preliminary data, and submit a grant proposal. With application success rates below 10% nowadays, this option is not for the feint of heart. It really requires a genuine interest in bench research and a willingness to pick yourself up off the canvas and dust off after each rejection until you finally break through. You'll also be doing seven postgraduate years of training after medical school (one internal medicine, three neurology, two NP, one AP).
A guest post regarding an important development from Dr. Olaf Bartsch:
The German company Dianova now provides reliable highly pure (goat anti-mouse chromatography) lyophilizates of antibody clone H09. The antibody has been purified from cellculture supernatants by GAM (goat anti-mouse) affinity chromatography resulting in a more intense staining of oligodendroglioma versus a clear negative reaction with glioblastoma.
Dianova's proprietary antibodies are now available in the USA directly and can be ordered from U.S. and Canadian customers on the HistoBioTec website or by purchase order.
Double staining of GFAP (red) and clone H09 (brown) of oligodendrogliopma infiltrating zone demonstrating specific labelling of tumor cells but not GFAP positive reactive astrocytes.
Antibody clone H09 serves as a Tumor Cell Marker for Astrocytoma and Oligodendroglioma and is highly usefull for the differentiation of reactive gliosis from low grade glioma. Moreover, the antibody differentiates single infiltrating tumor cells from reactive gliosis.
Fig.2
Infiltrating zone of anaplastic astrocytoma with specific labelling of infiltrating glioma cells by antibody clone H09.
Clone H09 was developed for staining of standard formalin-fixed paraffin embedded (FFPE) sections in clinical routine and is the first commercially available antibody that specifically stains single cells carrying the IDH1R132H point mutation.
Fig.3
Cortex infiltrated by oligodendroglioma with specific labelling of tumor cells by antibody clone H09.
If you like to discuss any issues regarding application of this unique antibody, you are welcome to visite our booth at the ICN 2010 (XVIIth International Congress of Neuropathology), September 11-15 in Salzburg.